Evidence
Clinical evidence for CorteXR Stroke.
The evidence summarised here relates to CorteXR Stroke and predecessor regulated clinical work in cognitive stroke rehabilitation after stroke. It should be read in the context of the published study, the intended use, and local clinical review.
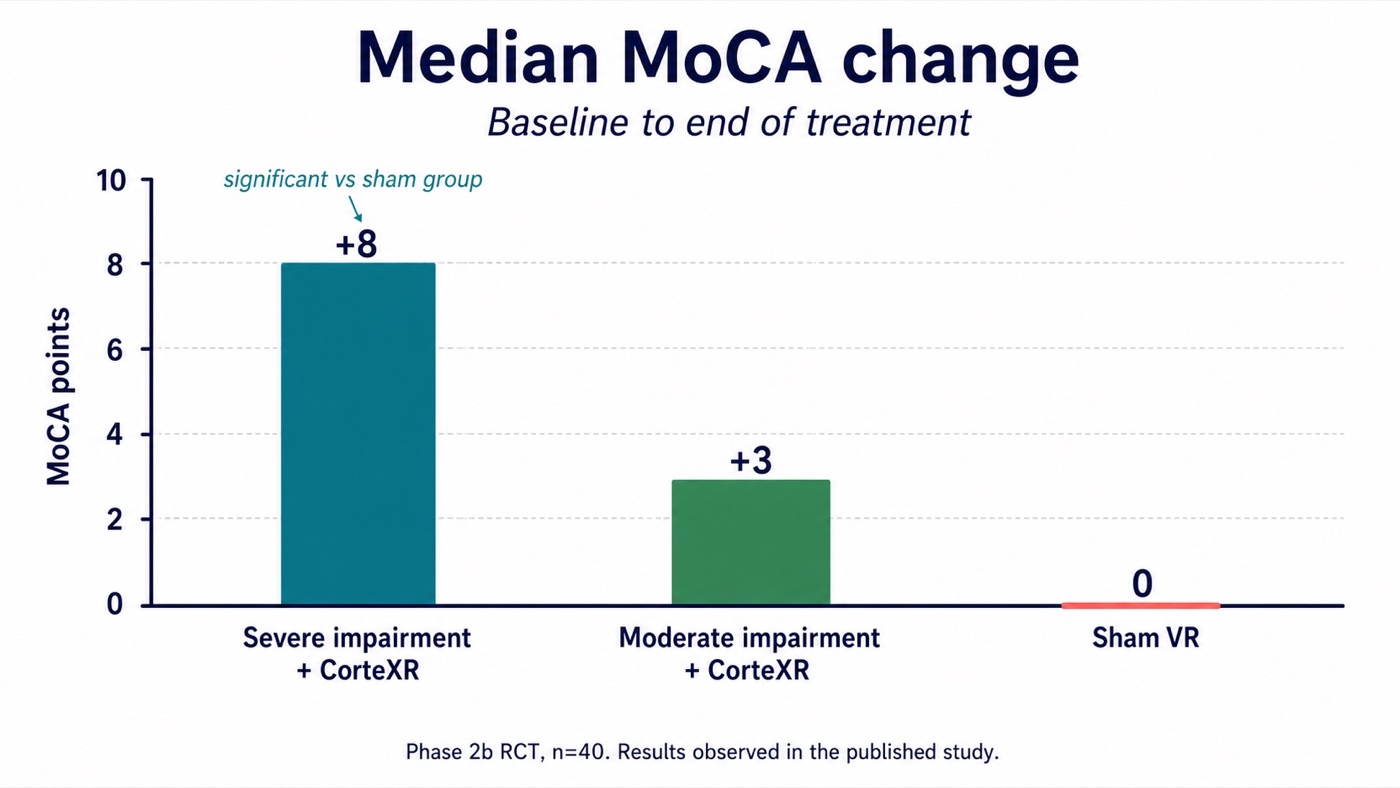
+8Reported median MoCA change in one subgroup
5 daysReported length-of-stay difference versus sham VR
0Serious adverse events reported
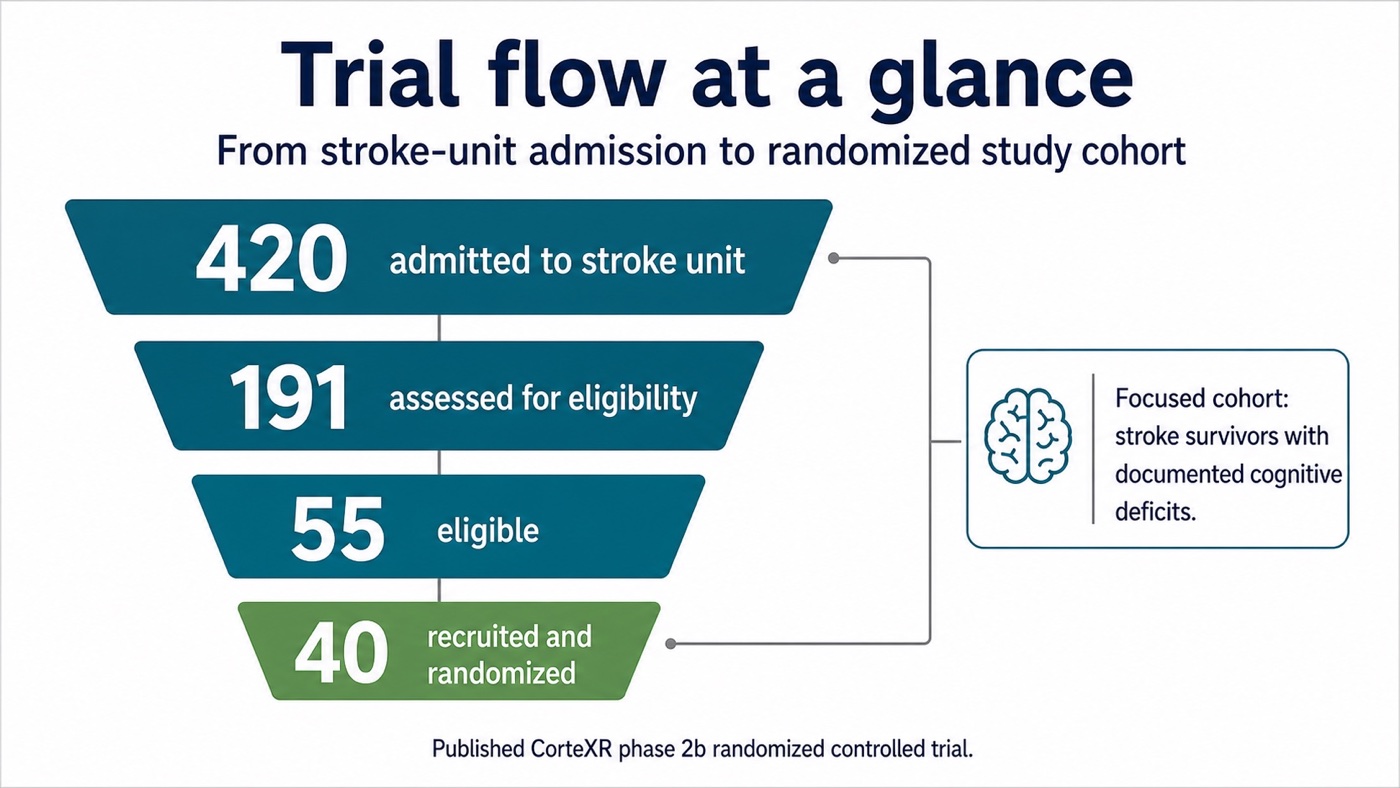
40Stroke survivors in phase 2b RCT
Reported in the published VIRTUE study. These figures are not claims for CorteXR Studio.